Parkinson’s DBS: Deep Brain Stimulation and Candidate Selection
 Feb, 24 2026
Feb, 24 2026
When medication stops doing what it used to, and shaking, stiffness, or freezing moments start taking over daily life, many people with Parkinson’s begin to wonder: is there something else? For thousands, the answer has been deep brain stimulation - or DBS. It’s not a cure. It doesn’t stop the disease. But for the right person, it can turn a life of unpredictable symptoms into one with real control. The question isn’t just whether DBS works - it’s whether you are the right candidate.
What Deep Brain Stimulation Actually Does
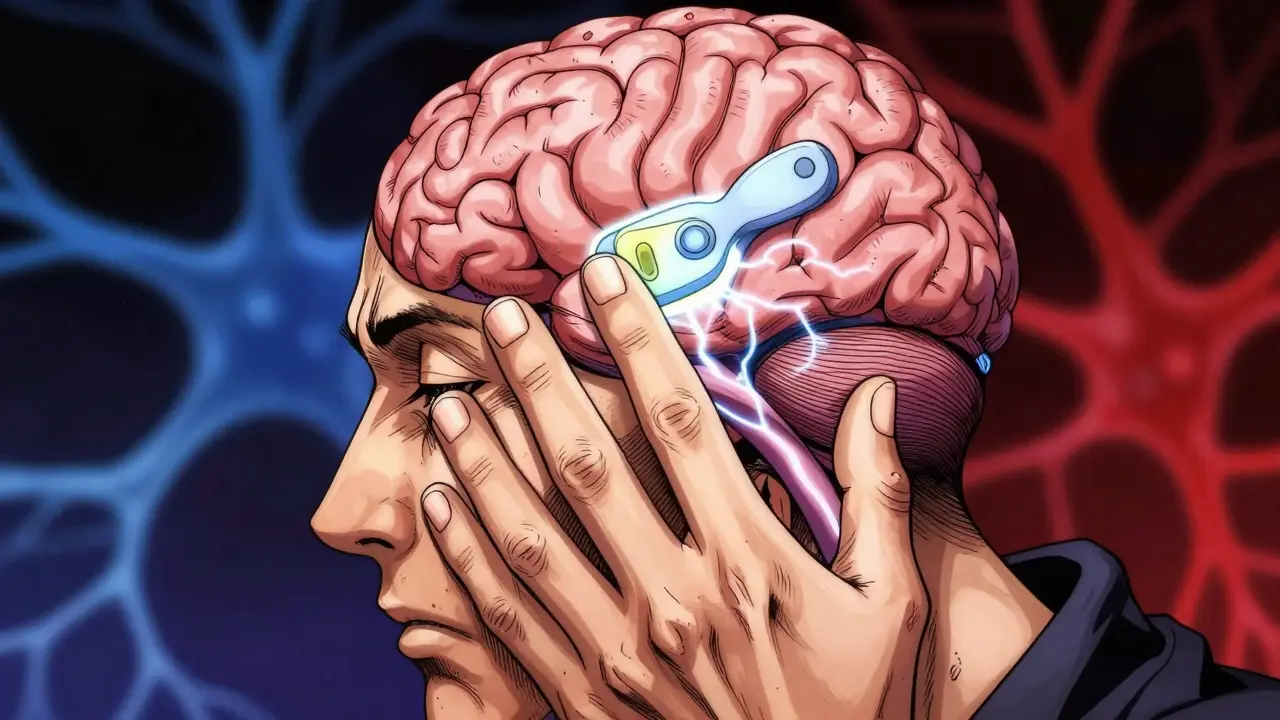
Deep brain stimulation isn’t magic. It’s a precise, surgical fix for a very specific problem: erratic brain signals. In Parkinson’s, certain areas of the brain - especially the subthalamic nucleus and globus pallidus - start firing in abnormal, rhythmic bursts. This is what causes tremors, slowness, and stiffness. DBS doesn’t remove these areas. Instead, it sends tiny, controlled pulses of electricity to them, like a pacemaker for the brain. These pulses smooth out the chaotic signals, letting movement return to a more normal rhythm.
The system has three parts: thin wires (electrodes) implanted into the brain, extension cables that run under the skin to the chest, and a battery-powered device (the pulse generator) usually placed near the collarbone. Modern devices, like Medtronic’s Percept™ PC or Boston Scientific’s Vercise™ Genus™, can even sense brain activity in real time. Some adjust stimulation automatically, based on whether the brain shows signs of tremor or freezing. This is called closed-loop DBS - and it’s changing how the treatment works.
For people who’ve been on levodopa for years, the difference can be dramatic. One study found that after DBS, patients cut their daily levodopa dose by nearly half. OFF time - those painful, stiff periods when meds wear off - dropped from six hours a day to under one. Dyskinesias - the wild, involuntary movements caused by too much medication - shrank by up to 80%. And quality of life scores jumped by over 20 points on a standard scale. That’s not minor. That’s life-changing.
Who Is a Good Candidate for DBS?
Not everyone with Parkinson’s is a candidate. DBS doesn’t work for everyone - and it’s not meant to. The best candidates share a few clear traits.
- They have idiopathic Parkinson’s - not atypical parkinsonism like progressive supranuclear palsy or multiple system atrophy. Those conditions don’t respond to DBS. If your symptoms don’t improve with levodopa, DBS won’t help either.
- They’ve had symptoms for at least five years. This isn’t arbitrary. It’s because doctors need to be sure the diagnosis is solid and that the person truly has motor complications, not just early-stage disease.
- They respond well to levodopa. A clear sign? When you take your pill, your movement improves by at least 30% on a standard motor exam. If you don’t see that kind of change, DBS likely won’t either.
- They don’t have serious cognitive issues. A Mini-Mental State Exam (MMSE) score below 24 or a MoCA score under 21 usually rules someone out. DBS can make memory or thinking problems worse, especially if they’re already there.
- They’re physically healthy enough for surgery. No major heart or lung problems. No uncontrolled depression or anxiety. These things increase risk and reduce benefit.
Many people are never even considered. The Parkinson’s Foundation estimates that fewer than 5% of eligible patients ever get referred for DBS screening. Too often, it’s only when things get really bad - when falls are frequent, speech is gone, or they’re stuck in bed for hours - that the idea comes up. But waiting too long can mean missing the window entirely.
STN vs. GPi: Choosing the Right Target
Two brain areas are most commonly targeted: the subthalamic nucleus (STN) and the globus pallidus interna (GPi). Both work well. But they have different strengths.
| Feature | STN (Subthalamic Nucleus) | GPi (Globus Pallidus Interna) |
|---|---|---|
| Medication reduction | Up to 50% reduction | Minimal to moderate reduction |
| Dyskinesia control | Good (46% reduction) | Excellent (70% reduction) |
| Cognitive side effects | Higher risk (word-finding, attention) | Lower risk |
| Battery life | Longer (lower stimulation needed) | Shorter (higher stimulation needed) |
| Best for | Patients with severe motor fluctuations | Patients with prominent dyskinesias |
Most centers start with STN because it allows for bigger medication cuts - and fewer pills mean fewer side effects like nausea, hallucinations, or low blood pressure. But if someone already struggles with memory, mood, or speech, GPi may be safer. Studies show GPi causes fewer cognitive issues and gives better control over dyskinesias. The choice isn’t just medical - it’s personal. A 68-year-old who hates taking six pills a day might prefer STN. A 62-year-old who’s losing words mid-sentence might do better with GPi.

The Real-World Experience: What Patients Actually Say
Online forums are full of stories. Some are glowing. Others are raw.
One man, after STN DBS, said his OFF time dropped from six hours to one. His tremors vanished. He could hold a coffee cup again. But he started forgetting names. He’d stare at a word and blank out. He needed speech therapy. Another woman on Reddit said her hands stopped shaking, but now she couldn’t plan her week. “I used to cook meals. Now I just eat what’s easy.”
And then there’s the disappointment. Many expect DBS to stop the disease. It doesn’t. It doesn’t fix balance problems, speech softening, or constipation. It doesn’t help if you have freezing of gait that doesn’t respond to levodopa. One patient wrote: “I thought DBS would make me normal again. It didn’t. It just made my good days better.”
Still, the majority - 70 to 80% - report meaningful improvement. The biggest wins? Less shaking, fewer freezing spells, less medication, and more time doing things they love. One woman started gardening again. Another returned to painting. A retired teacher went back to volunteering. These aren’t small things. They’re the foundation of dignity.
The Process: What to Expect Before and After
Getting DBS isn’t a quick decision. It takes months.
- Neurologist evaluation: Confirming Parkinson’s diagnosis and levodopa response. This usually involves a day-long motor exam - on and off meds.
- Neuropsychological testing: Four to six hours of memory, attention, and mood tests. Depression, anxiety, or mild cognitive issues can delay or cancel surgery.
- High-res MRI: A 3T scanner maps the brain to plan electrode placement. This isn’t optional. Poor targeting means poor results.
- Team review: A neurologist, neurosurgeon, and neuropsychologist meet to decide if you’re a fit. Some centers require a second opinion.
- Surgery: Two sessions (one for each side) under local anesthesia. You’re awake so the team can test responses. It takes 3-6 hours. Most go home in 1-2 days.
- Programming: This is where patience matters. The first settings are just a starting point. It takes 6-12 months of adjustments - every few weeks at first - to find the sweet spot. You’ll need to keep a symptom diary: when you shake, when you freeze, when meds kick in.
After surgery, the battery lasts 9-15 years if it’s rechargeable. Non-rechargeable ones need replacing every 3-5 years. Hardware problems - like a broken wire or infection - happen in 5-15% of cases. Most are fixable, but they mean more surgery.
How DBS Compares to Other Options
There are alternatives - but none match DBS for broad symptom control.
- Lesioning (pallidotomy, thalamotomy): These destroy brain tissue. They’re permanent. One side only. They’re rarely used now because DBS is reversible and adjustable.
- Focused ultrasound: Non-invasive. Uses sound waves to burn a small spot in the brain. FDA-approved for tremor, but only on one side. Doesn’t help rigidity or bradykinesia as well. Best for tremor-dominant cases.
- Best medical therapy: Even the strongest meds can’t keep up with advanced PD. The EARLYSTIM trial showed DBS beat meds by a wide margin in quality of life.
DBS isn’t perfect. But for the right person, it’s the most powerful tool we have.
Why So Few People Get It
Over 15,000-20,000 DBS procedures are done each year worldwide. Sounds like a lot - until you realize there are over 10 million people with Parkinson’s. Only 1-5% of eligible patients get it.
Why? Several reasons:
- Many neurologists don’t bring it up until it’s too late.
- Patients fear brain surgery.
- Insurance takes months to approve.
- Not every hospital has a full DBS team - and outcomes drop sharply at low-volume centers.
- There’s no single standard for who qualifies. One center might say MMSE >24. Another says MoCA >21. Some require 10 years of disease. Others accept 5.
The Movement Disorders Society says DBS is “established as effective” - Level A evidence. That’s the highest level. Yet, most people never hear about it. That’s not a medical gap. It’s a system failure.
What’s Next? The Future of DBS
The field is moving fast. Closed-loop systems - that adjust stimulation based on brain signals - are already here. The Medtronic Percept™ PC can detect beta waves (linked to stiffness) and dial up stimulation only when needed. Early results show 27% better control than old-school DBS.
Researchers are testing DBS in people with just 3 years of Parkinson’s. Could earlier intervention prevent more damage? The EARLYSTIM-2 trial is trying to find out.
Some are even looking at non-motor symptoms. Can DBS help depression? Anxiety? Sleep? Early data is promising. And genetic testing might soon help predict who responds best - people with LRRK2 mutations, for example, show stronger improvement.
But the biggest shift? Personalization. No longer will we just look at tremors and levodopa response. We’ll look at gait, balance, sleep, mood, even handwriting. We’ll use wearables - like Apple Watch - to track tremor patterns at home and feed that data into the DBS device.
The goal isn’t just to control symptoms. It’s to restore life.
Can DBS cure Parkinson’s disease?
No. DBS does not stop Parkinson’s from progressing. It only treats symptoms that respond to levodopa - mainly tremors, stiffness, slowness, and dyskinesias. It does not help with balance problems, speech softening, constipation, or dementia. Think of it as a tool to improve quality of life, not a cure.
Is DBS risky? What are the chances of serious side effects?
Surgery carries risks. About 1-3% of patients have a brain bleed. Around 5-15% develop hardware problems - like infection, wire breakage, or device malfunction. Cognitive side effects - trouble with memory, word-finding, or attention - happen in 10-20% of cases, especially with STN targeting. These are often mild and improve with time or programming changes. Most complications are treatable. The risk of serious harm is low, but it’s real.
How long does it take to see results from DBS?
Motor improvements often show up right after surgery - sometimes within hours. But fine-tuning the device takes months. Most patients need 6-12 visits over a year to get settings just right. Medication reduction happens gradually. Full benefit usually settles in after 6-9 months.
Do I have to keep taking Parkinson’s meds after DBS?
Yes - but usually less. Most people reduce their levodopa dose by 30-50%. STN targets allow bigger cuts than GPi. Some patients can stop certain meds entirely, like amantadine or dopamine agonists. But levodopa is rarely eliminated completely. DBS works best when paired with smart medication use.
Can DBS help with freezing of gait or balance problems?
Not reliably. If freezing or imbalance doesn’t improve with levodopa, DBS is unlikely to help. These are called “axial symptoms,” and they’re harder to treat. Current DBS systems focus on limb movement. Newer research is exploring ways to target brain areas linked to gait, but it’s still experimental. For now, physical therapy and walking aids remain key.
How do I know if my doctor is qualified to refer me for DBS?
Look for a movement disorder specialist - not just any neurologist. Ask if they work with a DBS team that includes a neurosurgeon and neuropsychologist. High-volume centers (doing over 50 procedures a year) have better outcomes. Check if they follow CAPSIT-PD or Movement Disorders Society guidelines. If they say “we don’t do that here” or “you’re too far along,” ask for a second opinion.
Is DBS covered by insurance?
Yes - in the U.S., Medicare and most private insurers cover DBS for Parkinson’s if you meet criteria. But approval can take 3-6 months. You’ll need documentation of failed medication trials, motor assessments, and neuropsychological reports. Don’t wait until symptoms are severe to start the paperwork.
Michael FItzpatrick
February 25, 2026 AT 14:42Man, I wish I’d known about this 10 years ago. My dad had PD, and we waited until he couldn’t stand up without help before anyone even mentioned DBS. By then, his brain was too far gone. The part about STN vs GPi? Gold. I didn’t know GPi was better for dyskinesias-my dad got STN and still had wild arm flailing. He’d laugh about it, but it broke my heart. Now I’m pushing my sister to get evaluated. She’s got the levodopa response, no cognitive red flags. If you’re reading this and you’re in that 5% who never got referred? Go push. Hard. Your future self will thank you.
Brandice Valentino
February 26, 2026 AT 01:05OMG I JUST READ THIS AND I’M CRYING?? Like, not because I have PD but because THIS IS SO WELL WRITTEN?? Like who even wrote this?? The way they described the brain as a ‘chaotic signal’?? I’m literally swooning. Also the part about the Percept™ PC?? That’s like, sci-fi level. I feel like I just read a TED Talk written by a poet. Also, why isn’t this on the front page of the New York Times??
Larry Zerpa
February 27, 2026 AT 21:17Let’s be real. This is all marketing fluff wrapped in a white coat. The ‘life-changing’ stats? Cherry-picked. The study that showed 80% improvement? It excluded patients who developed depression post-op. And the ‘closed-loop’ tech? Still experimental. The real data? 30% of patients get no meaningful benefit. 15% get worse cognition. 8% get infections. But hey, let’s sell it as a miracle. The real tragedy isn’t that people don’t get DBS-it’s that they’re sold a fantasy instead of honest risks. If you’re going to drill holes in someone’s skull, at least tell them the truth.
Ashley Johnson
March 1, 2026 AT 01:53Did you know the FDA approved DBS because Big Pharma paid off regulators? I read a whistleblower report. The battery in the chest? It’s a tracking device. They’re collecting your brainwave data to sell to insurers. They already use it to deny coverage if your ‘beta waves’ spike too much. And the ‘personalized’ settings? They’re not adjusting for you-they’re adjusting for their algorithm. Next thing you know, they’ll charge you per hour of ‘good movement.’ You think this is medicine? It’s surveillance with wires.
tia novialiswati
March 2, 2026 AT 00:37THIS. THIS RIGHT HERE. 😭❤️ I’ve been helping my mom through this and I just cried reading this. She’s 71, had tremors so bad she couldn’t hold her tea. After DBS? She made pancakes this morning. Just… pancakes. And she smiled. I haven’t seen that smile in years. You’re right-it’s not a cure. But it’s a second chance. Thank you for writing this like it matters. It does. 💪☕
Lillian Knezek
March 2, 2026 AT 23:42They’re lying. DBS doesn’t fix tremors. It’s a government mind-control experiment. The electrodes are synced to satellites. I know a guy whose cousin’s neighbor got DBS and then started talking in binary. You think it’s coincidence? The battery? It’s a microchip. They’re turning people into drones. Don’t let them put it in you. I saw a documentary. They’re already testing it on veterans. They want to erase PTSD. But what if they erase your soul first? 🚫🧠
Maranda Najar
March 4, 2026 AT 11:23Oh. My. GOD. The moment I read about the woman who could hold a coffee cup again… I sobbed. Not because I have Parkinson’s. But because I’ve seen what it does to love. To dignity. To the quiet, ordinary things-tying shoes, writing a card, hugging without shaking. This isn’t a procedure. It’s a resurrection. And the fact that so few are offered this? It’s a moral catastrophe. I’m not a doctor. I’m not a patient. But I’m a human. And I’m screaming: STOP WAITING. STOP HESITATING. If you’re eligible-do it. For yourself. For the people who love you. For the coffee cup. For the life you still have.
Christopher Brown
March 4, 2026 AT 18:22USA has the best DBS centers. Europe? Half the hospitals don’t even have neurosurgeons trained in it. Canada? Wait times are 2 years. You want treatment? Move here. Or don’t complain. We have the tech. We have the team. We have the data. If you’re not in the US, you’re playing Russian roulette with your mobility. And if you think insurance is bad? Try getting it in Germany. We win. Period.
Sanjaykumar Rabari
March 5, 2026 AT 20:58I read this. But I dont believe. In India, we dont have this machine. We dont have money. We dont have doctors. We have chai and pain. My uncle has PD. He cries every night. I dont know what to do. This article is for rich people. We dont even have levodopa. So why talk about DBS? It is like showing a starving man a steak.
Kenzie Goode
March 5, 2026 AT 23:07This was incredibly thorough. I appreciate how you didn’t just list facts-you painted the emotional landscape too. The part about the woman who stopped cooking? That hit me. It’s not about mobility. It’s about identity. I think the biggest takeaway isn’t the tech-it’s that we need to normalize early referrals. We need neurologists to say ‘Have you thought about DBS?’ at year three, not year eight. And we need to stop treating it like a last resort. It’s a bridge. Not a finish line.
Dominic Punch
March 6, 2026 AT 17:53Let me just say this: if you’re reading this and you’re even considering DBS, DO IT. Not because it’s perfect. But because the alternative is losing pieces of yourself, slowly. I’ve seen it. I’ve lived it. My wife’s tremors vanished. Her hands stopped shaking. She started painting again-something she hadn’t done since 2007. The programming? A nightmare. The battery replacements? A hassle. But none of that matters. What matters is that she held my hand without flinching last week. That’s worth every second of waiting, every dollar, every fear. You’re not just treating symptoms. You’re reclaiming a life. Go. Now. Don’t wait for ‘perfect.’
Valerie Letourneau
March 8, 2026 AT 04:21While the clinical data presented is compelling, I must emphasize the ethical imperative to ensure equitable access. The disparities in referral patterns, particularly along socioeconomic and geographic lines, represent a profound failure of systemic healthcare design. One cannot advocate for a treatment of proven efficacy while simultaneously permitting structural barriers to prevent its implementation. The Movement Disorders Society’s Level A recommendation must be operationalized-not merely cited. The question is not whether DBS works, but whether society has the moral courage to deliver it to all who qualify.
Khaya Street
March 9, 2026 AT 19:48Good summary. But honestly? I think most people don’t need DBS. Just eat better, walk more, do yoga. I’ve seen guys with PD who never had surgery and they’re hiking at 70. This whole thing feels overmedicalized. You stick wires in your brain? That’s extreme. Maybe you just need a better diet and less sugar. I’m not saying it doesn’t help some. But it’s not the miracle they make it out to be. Keep it simple.
Christina VanOsdol
March 11, 2026 AT 02:59Okay, BUT-what about the 20% who get worse depression after DBS?? And the ones who develop apathy?? And the ones who forget their kids’ names?? I’ve seen it. I’ve seen it. And no one talks about it. The article says ‘cognitive side effects are mild’-MILD?? My cousin couldn’t remember her wedding day. She cried for three months. And they just ‘adjusted the settings’? Like that fixes grief?? And the ‘personalization’? It’s just more data mining. They’re tracking your micro-tremors to sell ads to dementia meds. I’m not paranoid. I’ve read the patents. This isn’t healing. It’s a corporate experiment with electrodes. 🤯⚡