Therapeutic failures: when a generic drug doesn't work as expected
 Mar, 7 2026
Mar, 7 2026
When you’re prescribed a generic drug, you expect it to work just like the brand-name version. After all, regulators say they’re the same. But for some patients, that’s not true. A generic drug can fail - not because the disease got worse, not because the body changed, but because the pill in the bottle didn’t deliver what it promised. And when that happens, the consequences aren’t just inconvenient. They can be deadly.
What does "therapeutic failure" really mean?
Therapeutic failure means the drug didn’t do what it was supposed to. You take it. You follow the instructions. But your condition doesn’t improve - or worse, it gets worse. For someone on warfarin to prevent blood clots, that could mean a stroke. For a transplant patient on tacrolimus, it could mean organ rejection. For a cancer patient on chemotherapy, it might mean the tumor keeps growing while doctors think the treatment is working. The problem isn’t always the active ingredient. It’s everything else: how the pill breaks down, how fast it releases the medicine, how stable it stays on the shelf. These are called formulation differences. And they matter more than most people realize.The bioequivalence loophole
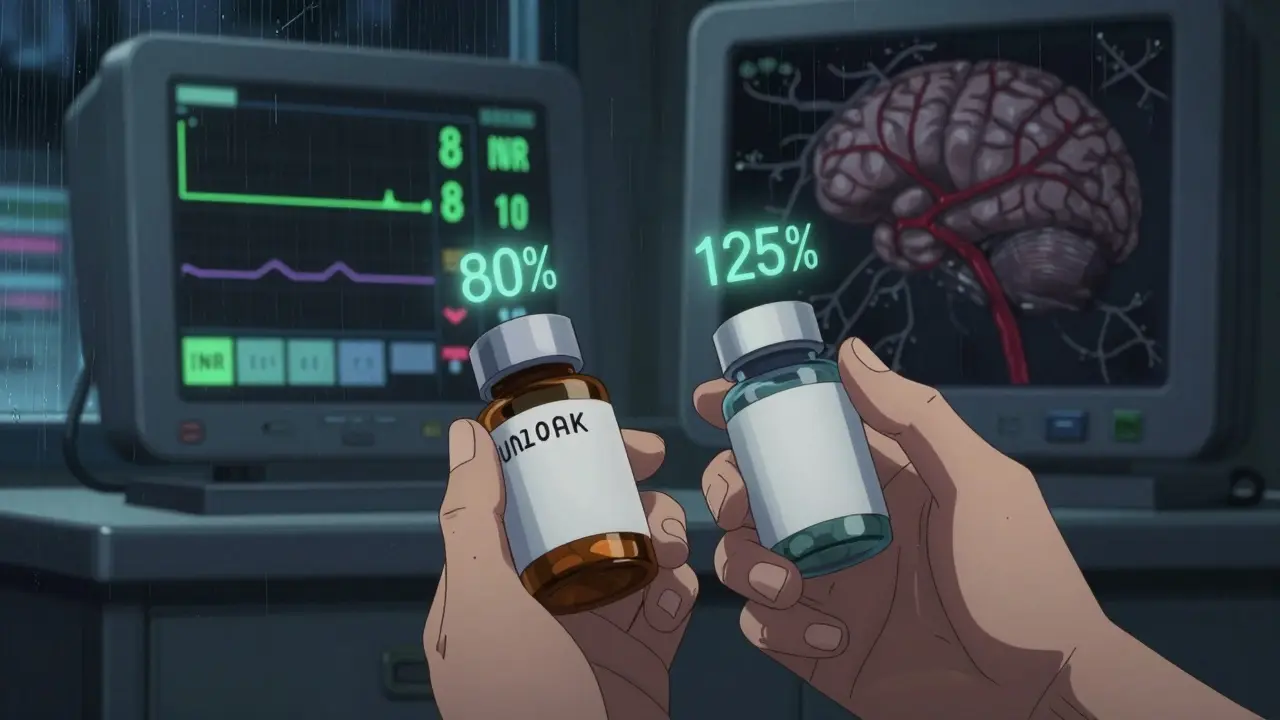
The FDA says a generic must be "bioequivalent" to the brand-name drug. That sounds solid. But here’s what that actually means: the generic’s absorption in your body can be as low as 80% or as high as 125% of the original. That’s a 45% range. For most drugs, that’s fine. But for drugs with a narrow therapeutic index (NTI), it’s a gamble. NTI drugs include:- Warfarin (blood thinner)
- Phenytoin (seizure control)
- Digoxin (heart rhythm)
- Tacrolimus (organ transplant rejection prevention)
- Lithium (bipolar disorder)
When the pill doesn’t dissolve right
A 2024 investigation by the Therapeutic Investigations Bureau of Journalism (TBIJ) found something shocking: pills from the same blister pack had wildly different amounts of active ingredient. One tablet had 97% of the labeled dose. The next had 72%. That’s not a manufacturing error. That’s systemic. Take Budeprion XL, a generic version of Wellbutrin. Patients started reporting severe mood swings, anxiety, and suicidal thoughts in 2008. The FDA finally pulled it off the market in 2013 - not because the active ingredient was wrong, but because the inactive ingredients changed how the drug released. The original used a slow-release coating. The generic used a different polymer. Result? The drug dumped all at once instead of over 12 hours. Patients got spikes of side effects, then no drug at all. Same thing happened with generic Concerta. Some versions released medication too fast. Others didn’t release enough. Kids with ADHD went from focused to lethargic - not because their condition changed, but because the pill didn’t work the way it was supposed to.
The silent threat: degradation and contamination
Medicines don’t stay perfect forever. Heat, humidity, light - they all break down active ingredients. A pill sitting in a warehouse in India or Bangladesh might be fine when shipped. But after months in a hot warehouse in the U.S., or sitting in a patient’s bathroom cabinet, it can lose 20% of its potency. In 2025, STAT News reported that over 30% of failed generic drugs tested contained less than 88% of the labeled active ingredient. Some had more than 112%. Both are dangerous. Too little? Treatment fails. Too much? Toxicity kicks in. And then there’s contamination. Valsartan, a common blood pressure drug, was recalled in 2018 after nitrosamine impurities were found - cancer-causing chemicals. Losartan and irbesartan followed. Ranitidine (Zantac) was pulled because of NDMA, another carcinogen. These weren’t mistakes. They were preventable.Who’s responsible? The broken supply chain
The generic drug market is a global mess. Over 80% of active pharmaceutical ingredients (APIs) come from India and China. Regulatory oversight varies wildly. One factory might pass a U.S. inspection. The next one down the road? No one checks. Pharmacy Benefit Managers (PBMs) - the middlemen who negotiate drug prices for insurers - often push for the cheapest generic, regardless of quality. They get rebates from manufacturers. Patients get the lowest price tag. But when that cheap generic fails, the patient pays the real cost: hospital visits, missed work, organ failure. A 2023 study from the USC Schaeffer Center found that PBMs profit more when generics are cheap and unreliable. Why? Because when a patient’s drug fails, they get switched to a new one - often a more expensive brand-name version. The PBM gets a rebate again. The cycle repeats.Real stories, real damage
A heart transplant patient in Bristol, UK, noticed her fatigue getting worse. Her doctors thought it was rejection. But her blood levels of tacrolimus were dropping. She’d been switched to a generic. Testing revealed the tablets contained only 81% of the labeled dose. She switched back to the brand name. Within weeks, her energy returned. A woman in her 60s on warfarin for atrial fibrillation had a stroke. Her INR - a measure of blood thinning - was dangerously low. Her generic had been changed twice in six months. Lab tests showed inconsistent absorption. She now insists on the brand name. Her doctor agrees. In 2024, Glenmark Pharmaceuticals recalled nearly 47 million doses of potassium chloride because the tablets didn’t dissolve properly. Patients with low potassium - often elderly, with heart conditions - were at risk of cardiac arrest. The recall came too late for some.What you can do
If you’re on a drug with a narrow therapeutic index - or if your condition suddenly worsens after switching to a generic - don’t assume it’s your body. Ask:- Which generic version am I taking? (Check the label - manufacturers change often)
- Has my pharmacy switched my prescription without telling me? (They can, legally, unless your doctor blocks it)
- Can I request the brand-name version? (Many insurers will approve it if you prove the generic failed)
- Have my blood levels been checked since the switch? (For warfarin, lithium, digoxin - they should be)
The bigger picture
The system isn’t broken because of bad actors. It’s broken because profit comes before precision. The same companies that make brand-name drugs also make the generics - often in different factories, with different quality controls. The FDA approves them based on outdated standards. Regulators in other countries have even looser rules. Patients are being told, "It’s the same." But it’s not. Not always. Not for the drugs that need to be perfect. The FDA is slowly tightening rules for NTI drugs. But change moves slower than patients die. Until then, vigilance is your best defense.Can a generic drug really be less effective than the brand name?
Yes. While most generics work fine, some - especially those with a narrow therapeutic index - can differ in how they’re made. Differences in inactive ingredients, dissolution rates, or active ingredient stability can cause the drug to be absorbed too slowly, too quickly, or not at all. This doesn’t mean the generic is fake. It means it’s not therapeutically equivalent in practice, even if it passes regulatory tests.
Which drugs are most at risk for therapeutic failure?
Drugs with a narrow therapeutic index (NTI) are most at risk. These include warfarin, phenytoin, digoxin, lithium, cyclosporine, tacrolimus, and levothyroxine. Even small changes in blood levels can lead to serious side effects - from organ rejection to seizures to stroke. Chemotherapy drugs and some antidepressants also show troubling variability in real-world use.
Why do pharmacies switch my generic without telling me?
Pharmacies often switch generics to the cheapest option available, which can change monthly based on contracts with distributors. This is legal unless your doctor specifically writes "dispense as written" or "no substitutions." Many patients don’t realize their prescription was switched - until they start feeling worse.
How can I check if my generic drug is safe?
Check the manufacturer name on the pill bottle. Look up recalls on the FDA website (or your country’s equivalent). Ask your pharmacist if the generic has had recent quality issues. For NTI drugs, request blood level monitoring (like INR for warfarin) after any switch. If symptoms change after a switch, report it to your doctor immediately.
Should I always choose brand-name drugs over generics?
Not necessarily. For most drugs, generics are safe and effective. But if you’re on a drug with a narrow therapeutic index - or if you’ve had a bad reaction after switching - ask your doctor to prescribe the brand name. Many insurance plans will approve it if you document therapeutic failure. Your health is worth the extra cost.
Judith Manzano
March 8, 2026 AT 07:04I’ve been on warfarin for 8 years. Switched generics twice. Both times, my INR dropped like a rock. No warning. No explanation. Just a trip to the ER and a scary night wondering if I’d stroke out. I now demand the brand. My doctor rolls his eyes, but he signs the paperwork. If your life depends on it, don’t gamble with pills labeled "same as brand". They’re not.
Also, check your pharmacy’s website - they often list the manufacturer. If it’s a name you don’t recognize, ask. You’re not being paranoid. You’re being smart.
rafeq khlo
March 8, 2026 AT 17:44The entire system is a farce. India and China produce 80 percent of APIs and yet we allow them to operate under regulatory standards that would be considered criminal in any developed nation. The FDA is a captive of corporate lobbying. They approve generics based on outdated bioequivalence thresholds that were never designed for NTI drugs. This is not negligence. This is systemic malfeasance. Patients are being sacrificed on the altar of profit. There is no moral high ground here. Only greed.
And yet we continue to trust the system. How naive. How tragic. How predictable.
Morgan Dodgen
March 8, 2026 AT 22:36Bro I saw this on a subreddit once and it blew my mind 😱
Turns out the "inactive ingredients" in generics are basically junk science. Like imagine your car’s engine is perfect but the fuel line is made of duct tape. That’s what happens. One guy in Ohio had a heart attack because his generic tacrolimus dissolved in 20 minutes instead of 12 hours. He was on the same dose. Same body. Same everything. Just a different polymer coating. And the FDA approved it. 😭
Also PBM rebates? Yeah they literally profit when you get sick. They get paid to switch you to a new drug after the cheap one fails. So they have incentive to let bad generics through. It’s not a bug. It’s a feature. 🤯
Stop trusting the system. Check your pill bottle. Google the manufacturer. If it’s Ranbaxy or Glenmark - run. Run fast.
Philip Mattawashish
March 9, 2026 AT 11:58You people are naive. You think this is about "quality control"? It’s about control. Period. The pharmaceutical-industrial complex doesn’t want you to know that the same company that made the brand-name drug also makes the generic - just in a different factory with cheaper workers, inferior equipment, and zero oversight. They don’t care if you die. They care if you keep buying. And they know you’ll keep buying because you don’t know the difference. You’re being gaslit by your own prescriptions.
There’s a reason why cancer patients in the U.S. are dying while their pills sit in warehouses in Chennai. The supply chain isn’t broken. It was designed this way. Profit > Precision > People.
Wake up. Your life is a commodity.
Tom Sanders
March 9, 2026 AT 14:29Bro I just switched to a generic for my antidepressant and now I feel like a zombie. Took me 3 weeks to realize it wasn’t me. My doc was like "oh yeah we switched". No warning. No nothing. Just a new pill. Now I’m back on brand. Worth every penny. Don’t be a hero. If your brain feels off after a switch - it’s not in your head. It’s in the pill.
Jazminn Jones
March 11, 2026 AT 13:43The notion that bioequivalence is sufficient for drugs with a narrow therapeutic index is not merely scientifically indefensible - it is an abdication of regulatory duty. The 80-125% range, originally established for non-critical medications, was never validated for anticoagulants, immunosuppressants, or antiepileptics. To permit interchangeability under these parameters is to institutionalize therapeutic uncertainty. The FDA’s continued failure to revise its guidelines for NTI drugs constitutes a breach of the social contract between public health authorities and the citizenry.
Moreover, the opacity of generic sourcing and the absence of mandatory batch-level disclosure render informed consent impossible. This is not healthcare. It is pharmacological roulette.
Erica Santos
March 12, 2026 AT 12:16So let me get this straight - we’ve turned medicine into a commodity, then let the cheapest bidder make it, then act shocked when people die because the pill didn’t dissolve properly? Wow. Truly groundbreaking. I mean, who knew capitalism applied to life-saving drugs would end in tragedy? 😏
Next up: Walmart starts selling "premium" insulin. Same active ingredient. Different color. Costs $20. You get a coupon for a free hospital visit if it doesn’t work. You’re welcome, America.
George Vou
March 14, 2026 AT 05:59my dr told me to switch to generic and now i feel like i got hit by a truck. i thought it was depression coming back. turns out my pill was just crap. pharmacy switched it without telling me. now i only take brand. no more "savings". my brain is worth more than $15.
also if your doc says "all generics are the same" theyre lying. or dont know what theyre talking about. either way dont trust em.